Types of Surgery
- LSG (Sleeve Gastrectomy)
Sleeve Gastrectomy (Fig. 1) includes removal of sleeve of stomach so that it can hold up to 50 to 150 ml of fluid depending on use of bougie size.
Sleeve gastrectomy is an irreversible procedure. The advantages of sleeve are that it removes the portion of stomach that produces hormone that stimulates hunger (Ghrelin). Dumping syndrome is less likely due to the preservation of the pylorus. By avoiding the intestinal bypass, the chance of intestinal obstruction (blockage), anemia, osteoporosis, protein deficiency and vitamin deficiency are significantly reduced. Very effective as a first stage procedure for high BMI patients (BMI >55 kg/m2) and limited results have shown promising as a single stage procedure for low BMI patients (BMI 35–45 kg/m2).
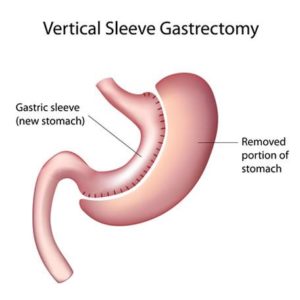
Figure 1
- LRYGB (Gastric bypass)
Laparoscopic Roux-en-Y gastric bypass (Figure 2) has mixed restrictive and malabsorptive component. It consists of forming a 25 to 30 cc pouch and bypass of 70 to 100 cm biliopancreatic limb and 100 to 130 cm of alimentary limb.
The advantage of gastric bypass is better weight loss and control of diabetes but it is associated with dumping syndrome, nutritional deficiencies, and others. The patients need to take life long multivitamins and minerals.
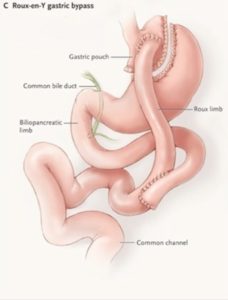
Figure 2
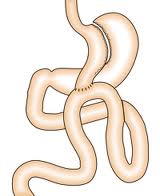
- Laparoscopic Mini Gastric bypass (LMGB)
Laparoscopic Mini Gastric bypass (Fig 3) consists of forming a long gastric tube and attaching it 180 to 200 cm down to small bowel with single anastomosis. Unlike conventional gastric bypass it has fewer early and long term complications and can achieve weight loss similar to it. The disadvantage is bile reflux which is mentioned but practically very few patients observe it.
If we compare the four procedures, the sleeve gastrectomy has advantages and disadvantages. It carries lesser risk than the bypasses, and has a faster weight loss.
As it does not involve any diverting or bypassing of the intestine, there is less likelihood that patients will require long term vitamin, mineral or protein supplements. Unlike the gastric bypasses, you have a normal gut anatomy and therefore can have standard diagnostic procedures such as Gastroscopy can be carried out postoperatively. There is no “dumping” with the sleeve gastrectomy as seen with the gastric bypasses and significant dietary change is not required as compared to the gastric band. However, unlike the gastric bypasses, the stomach is permanently removed. It is also possible to convert the sleeve gastrectomy into another weight loss procedure, usually a gastric bypass, if future problems arise. Once you are over the initial perioperative period, the likelihood of further problems with a gastric sleeve is low.
Please carefully weigh the advantages and disadvantages of each of the available bariatric procedures before you decide which you feel is the one for you. If I feel that a particular procedure has advantages for you, I will recommend that during our consultation.
- SILS (Scarless) Bariatric surgery
Now a day’s single incision surgery is gaining popularity and bariatric is no exception. Single incision bariatric surgery can be performed in selected subgroup of patients, young females with height less than 180 cm and no previous umbilical surgery.















